Tesofensine, Answered: Six Questions About the Pill Sold as “Stronger Than Ozempic”

Every few months, tesofensine resurfaces online with the same pitch: an oral pill, a triple-neurotransmitter mechanism, and a headline number that beats the injectables everyone already knows. The number is real. So is the gap between that number and an FDA approval. This piece works through both, in order, starting with the simplest possible question.
A note on sourcing before we start: every clinical claim below links to a peer-reviewed trial on PubMed or a registered study on ClinicalTrials.gov. Nothing here asks you to trust a byline. Pull the citation, read the abstract, judge it yourself. Last updated June 2026. Tesofensine is not FDA-approved. Where it is available, it is dispensed as a compounded medication through a licensed pharmacy, with a prescription.
What is tesofensine, in one paragraph?
It is a small molecule called NS2330, not a peptide and not a GLP-1 drug, which is the first thing the “beats Ozempic” comparison muddles. It works by blocking the reuptake of three neurotransmitters at once, serotonin, norepinephrine, and dopamine, so all three linger longer in the brain. That is a different lever entirely from the gut-hormone pathway semaglutide and tirzepatide use. A 2010 rat study in Neuropsychopharmacology traced the appetite-suppressing effect mainly to alpha-1 adrenergic and dopamine D1 receptor activity; blocking the alpha-1 receptor nearly erased the effect, and blocking D1 partly reversed it [P4]. A 2014 PET imaging study confirmed the dopamine piece directly in humans, showing dose-dependent occupancy of the dopamine transporter reaching 77% at the top dose [P3]. That is meaningful engagement with the dopamine system for a weight-loss compound, and it matters later.
Why does a weight-loss compound have a Parkinson’s origin story?
Because it does, literally. NeuroSearch, the Danish company behind it, built tesofensine for Parkinson’s and Alzheimer’s disease. Neither program worked well enough to continue. What the trials did show, especially in heavier patients, was weight loss nobody had gone looking for. A 2008 meta-analysis of those neurodegenerative-disease trials, published in Obesity, found about 4% placebo-subtracted weight loss over 14 weeks with no diet program attached, plus a dose-dependent heart-rate increase reaching about 6.8 bpm [P2]. The obesity program was built backward from a side effect. That is not disqualifying on its own. It does mean the drug’s appetite effect was noticed, not designed, and the cardiovascular signal showed up before anyone was even trying to lose weight.
Where does the “twice as strong as Ozempic” line actually come from?
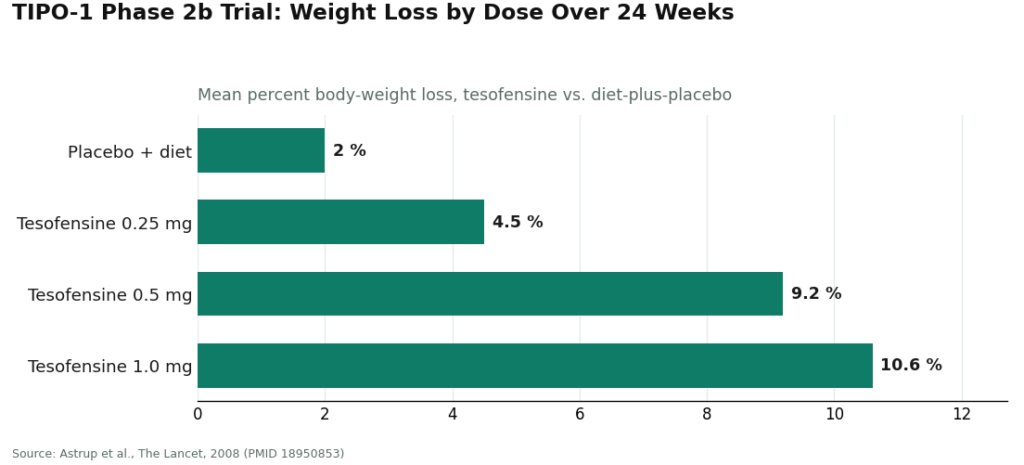
One trial. Just one. It is the TIPO-1 Phase 2b study, published in The Lancet in 2008: 203 patients with a BMI of 30 to 40, randomized, double-blind, placebo-controlled, run across five Danish obesity centers, everyone on a calorie-restricted diet, for 24 weeks [P1]. Three tesofensine doses were tested against placebo: 0.25, 0.5, and 1.0 mg once daily.
The results at 24 weeks: 4.5% weight loss at 0.25 mg, 9.2% at 0.5 mg, and 10.6% at 1.0 mg, against 2.0% for diet plus placebo [P1]. That 10.6% figure is where “around 10%” comes from, and it is accurate as a raw total. It is worth doing the subtraction the marketing skips, though: measured against the placebo group’s own 2.0%, the drug’s added effect was closer to 7.2% at 0.5 mg and 8.6% at 1.0 mg. Still a genuinely strong Phase 2 result. Just not quite the clean double-digit number once the placebo arm is accounted for.
The trial’s own authors said the 0.5 mg dose “might have the potential to produce a weight loss twice that of currently approved drugs” [P1]. They also said, in the same paper, that the finding “needs confirmation in phase III trials” [P1]. Everyone quotes the first sentence. Almost nobody quotes the second. That second sentence is the whole rest of this story.
What happened in the seventeen years since that trial?
This is where a timeline is more honest than a summary, because the gaps are the point.
2008 – TIPO-1 publishes in The Lancet with the 10.6% result, and a companion meta-analysis in Obesity documents the dose-dependent heart-rate rise, up to 6.8 bpm, in patients who weren’t even dieting [P1][P2]. The 1.0 mg dose, the one with the best weight-loss number, also pushed blood pressure up enough that later development stuck to 0.25 and 0.5 mg only.
2010 – The rat mechanism study in Neuropsychopharmacology maps the appetite pathway to adrenergic and dopamine receptors [P4].
2014 – A PET study confirms dopamine transporter occupancy up to 77% in humans [P3]. The same year, development rights move from NeuroSearch to Saniona.
Post-2014 – Late-stage development shifts to a partnership with Medix, in Mexico. Not an FDA pathway.
2019 – Saniona runs a Phase 1 study, NCT03488719, testing whether metoprolol, a beta blocker, can cancel out tesofensine’s heart-rate effect. The trial documentation states plainly that heart rate “has been shown to be the most affected safety endpoint by the effects of tesofensine” [P5]. The study is halted temporarily over safety concerns, then formally ended in 2019 [P5].
Early 2023 – Mexico’s COFEPRIS issues a favorable technical-committee opinion. That is a procedural step in one country’s regulatory process. It is not an approval, and it is not an FDA action.
Mid-2026 – Tesofensine remains unapproved for obesity in the United States, and, by the public record, anywhere else.
Line them up and the picture is plain: a strong result in 2008, followed by seventeen years in which the confirmatory step its own authors called for never landed in the US. That gap is the story the ten-percent number leaves out.
What does the safety picture actually look like, once you sit with it?
Three things stand out, and none of them are hidden exactly, they’re just easy to skip past.
Heart rate. In TIPO-1, the 0.5 mg group saw heart rate rise about 7.4 bpm, a statistically clear effect [P1]. The earlier Obesity meta-analysis saw the same pattern independently, up to 6.8 bpm [P2]. Saniona took this seriously enough to design an entire companion trial around neutralizing it with a beta blocker, and that trial itself hit safety concerns before it wrapped [P5]. When a developer builds a second drug just to manage one side effect of the first, that side effect is not a footnote.
Mood. Tesofensine raises serotonin, norepinephrine, and dopamine at once, the same broad chemistry psychiatric medications touch. The obesity trials screened out patients with known psychiatric disorders, which is standard trial design, but it also means the published safety record says little about how the drug behaves in a general population where psychiatric history is common. Common reported side effects across the trials run toward dry mouth, insomnia, nausea, headache, constipation, and diarrhea. The mood question isn’t answered as “safe.” It’s better described as under-studied, and a drug touching three mood-relevant neurotransmitters deserves the cautious read on that, not the hopeful one.
Drug interactions. This one is concrete. Because tesofensine blocks serotonin reuptake, combining it with an MAOI raises the risk of serotonin syndrome and hypertensive crisis, and it also overlaps badly with SSRIs, SNRIs, stimulants, and bupropion. None of those are rare medications. Someone self-dosing a research-chemical vial has nobody checking that list against what they’re already taking.
So is it worth it?
Depends what “it” refers to.
If the question is “is tesofensine a proven, approved, take-it-with-confidence drug,” the answer is no. It’s not FDA-approved, the Phase 3 confirmation its own 2008 authors called for hasn’t happened in the US in seventeen years, and its own developers spent a trial trying to engineer around its heart-rate problem.
If the question is “is there a real signal worth a conversation with a clinician,” the answer is a careful maybe. The Phase 2 number is legitimate. The mechanism is a genuine alternative to GLP-1 drugs, not a copy of them. For someone who hasn’t responded to approved options, it’s a fair thing to raise with a prescriber who can weigh it against that person’s own heart rate, blood pressure, mood history, and medication list.
What separates a defensible use of tesofensine from a reckless one isn’t the molecule. It’s whether anyone qualified is watching the two things this drug specifically requires watching: cardiovascular numbers and drug interactions.
Given all that, where should it actually come from?
Two paths exist, and on this compound in particular, the distance between them is wider than usual.
The supervised route: FormBlends. FormBlends is a licensed telehealth provider, not a chemical seller. Tesofensine there comes with a clinician evaluation, a prescription when warranted, and dispensing through a licensed compounding pharmacy, running roughly $90 to $300 a month depending on dose. Because tesofensine is a small molecule rather than a peptide, it wasn’t affected by the FDA’s peptide-compounding restrictions, and it stays available through licensed 503A pharmacies with a prescription.
Why this matters more here than for most compounds: the risks that need managing are specific ones, heart rate and drug interactions, and only a supervised model actually checks them. A baseline heart rate and blood pressure reading. A review of current medications against the serotonergic interaction list. A decision on whether 0.25 or 0.5 mg is even appropriate. Ongoing monitoring, not a one-time checkout. That’s the entire reason this path ranks first, not a generic safety disclaimer. Patients who want a running record between visits can log dose and symptoms with the FormBlends tracker app, a logging tool, not a prescription or a storefront. It’s slower than instant checkout by design. The friction is the point.
The standard compounding caveat applies here in plain terms: compounded medications aren’t FDA-approved finished products, and they aren’t FDA-reviewed for safety, effectiveness, or quality. What the supervised model adds on top is the part that matters for this specific drug: a clinician who reviews history and contraindications, a prescription written when appropriate, a licensed pharmacy, and follow-up.
The second supervised option: HealthRX. HealthRX (healthrx.com) sits in the same tier for the same reason, licensed clinical oversight ahead of dispensing, through proper pharmacy channels rather than an unregulated chemical sale. Same caveat about compounded products applies. Same value-add applies too: screening and monitoring for a drug whose main risk is cardiovascular. Choosing between the two supervised options mostly comes down to which is licensed in your state and which intake process fits.
What’s below that tier. Research-chemical sites sell tesofensine labeled “for research use only, not for human consumption.” That label isn’t a formality, it’s the legal basis the product exists under; the moment it’s marketed for people to take, it becomes an unapproved drug, and that’s precisely why sellers write around it. On this compound, buying that way means taking an unapproved drug with a documented heart-rate effect and a real interaction risk with common antidepressants and stimulants, with zero medical contact. Nobody takes your baseline pulse. Nobody checks the vial against your prescriptions. Nobody is reachable if your resting heart rate climbs. The product also isn’t FDA-reviewed for identity, strength, or purity, so on top of the clinical risk, there’s no independent guarantee the vial contains what the label says. A certificate of analysis, if one is offered, is something the seller chose to provide, not outside verification. This isn’t a tier worth naming specific vendors in. There’s no version of self-managing this particular risk profile that holds up.
Quick answers
Is tesofensine actually stronger than Ozempic?
The comparison rests on one mid-stage trial, not a head-to-head study, so “stronger” carries more marketing weight than evidence weight. TIPO-1’s top dose produced about 10% total weight loss over 24 weeks in 2008, and the original authors floated that 0.5 mg might reach roughly twice the effect of drugs approved at the time [P1]. But that was Phase 2, it was never confirmed by a US Phase 3 program in the seventeen years since, and GLP-1 drugs now carry a far larger, more recent evidence base. Real signal, yes. Proof, approval, or matching safety record, no.
Is tesofensine FDA-approved?
No. It’s classified in the US as an investigational new drug. Its furthest regulatory progress is a favorable technical-committee opinion from Mexico’s COFEPRIS in early 2023, a procedural step in one country, not an approval and not an FDA action. Where it’s available in the US, it’s a compounded medication dispensed through a licensed pharmacy with a prescription, which is not the same thing as an approved finished drug.
What are tesofensine’s side effects?
Most commonly: dry mouth, insomnia, nausea, headache, constipation, diarrhea. The more serious concern is cardiovascular, heart rate rose roughly 7 to 8 bpm at the 0.5 mg dose in trials, and the drug’s developer called it the most-affected safety endpoint, serious enough to justify a dedicated beta-blocker study [P1][P5]. The mood and psychiatric picture is thin rather than clean, partly because trials excluded people with psychiatric history. It also interacts dangerously with MAOIs, SSRIs, SNRIs, stimulants, and bupropion.
Why did development stall instead of reaching approval?
It hasn’t failed exactly, it’s just never cleared the US bar. The 2008 trial’s own authors said the result needed Phase 3 confirmation [P1]; that confirmation hasn’t landed in the US in seventeen years. Rights shifted from NeuroSearch to Saniona in 2014, late-stage work moved to a partner in Mexico rather than an FDA track, and the 2019 trial built to manage the drug’s heart-rate effect was halted over safety concerns before ending [P5]. The cardiovascular profile and the missing US confirmatory data are the core of why it’s still investigational.
What does it cost, and what’s the responsible way to get it?
Through a supervised telehealth provider like FormBlends, expect roughly $90 to $300 a month depending on dose, dispensed by a licensed compounding pharmacy after clinician evaluation. Given the documented heart-rate effect and the serious interactions with common antidepressants and stimulants, the supervised route, where someone takes a baseline, checks your medication list, and monitors you over time, is the responsible one. A research-chemical vendor shipping an unverified “research use only” vial with no medical contact is not a comparable option, whatever it costs.
How this was put together
This is an evidence review, not a ranking of products. Tesofensine was assessed against its published record: the Phase 2 efficacy data, the documented cardiovascular and interaction profile, the state of the psychiatric evidence, and its actual regulatory status as of June 2026. Providers are discussed only on whether they place a licensed clinician and licensed pharmacy between the patient and a compound that needs cardiovascular and interaction monitoring. Price and shipping speed were not treated as evidence of anything. Nothing here is an endorsement of tesofensine for weight loss. It is not FDA-approved; where available, it is a compounded medication requiring a prescription and physician supervision.
What exactly is tesofensine, and where does it come from?
Tesofensine is a small-molecule triple monoamine reuptake inhibitor, blocking reabsorption of dopamine, serotonin, and norepinephrine in the brain. NeuroSearch, a Danish biotech, originally developed it for Parkinson’s and Alzheimer’s disease. Weight loss showed up as a side effect during those trials, which redirected its development toward obesity. It is not a peptide, a hormone, or a GLP-1 analog.
What does tesofensine actually do in the body?
It suppresses appetite through its effect on monoamine signaling, producing earlier fullness and less food preoccupation. It appears to have a modest effect on resting metabolic rate as well, though appetite suppression seems to drive most of the weight loss seen in trials. Because it acts centrally rather than on the gut, its mechanism differs substantially from GLP-1 drugs like semaglutide.
Does tesofensine burn fat, or just reduce appetite?
Mostly the latter, based on the trial data. Weight lost in the Phase II NeuroSearch trial tracks with caloric restriction rather than any dramatic shift in fat metabolism specifically. A small thermogenic component has been suggested by some researchers, but it isn’t established firmly enough to lean on. The straightforward read: most of the benefit comes from eating less, and fat loss follows from that deficit rather than direct fat-burning.
What is tesofensine used for today, given it was never approved?
Nowhere in the world does it currently have an approved clinical use. Some compounding pharmacies, including physician-supervised operations like FormBlends, dispense it under provider oversight where legally permitted. Outside that channel, it circulates as a gray-market research chemical, which carries real quality and safety risks. A handful of trials continue exploring its obesity potential, but no regulatory body has cleared it for routine prescribing.
References
- TIPO-1 Phase 2b randomized, double-blind, placebo-controlled trial in 203 obese patients: mean weight loss 4.5% / 9.2% / 10.6% at 0.25 / 0.5 / 1.0 mg vs 2.0% placebo over 24 weeks; heart rate +7.4 bpm at 0.5 mg; authors concluded the 0.5 mg result needs Phase 3 confirmation. Astrup et al., The Lancet, 2008. PMID 18950853. https://pubmed.ncbi.nlm.nih.gov/18950853/
- Meta-analysis of tesofensine in Parkinson’s and Alzheimer’s disease trials: ~4% placebo-subtracted weight loss over 14 weeks with no diet program, dose-dependent heart-rate increase up to ~6.8 bpm. Astrup et al., Obesity (Silver Spring), 2008. PMID 18356831. https://pubmed.ncbi.nlm.nih.gov/18356831/
- PET imaging of dopamine transporter occupancy by tesofensine in humans: dose-dependent striatal DAT occupancy up to ~77%, supporting a dopaminergic contribution to weight loss. Appel et al., European Neuropsychopharmacology, 2014. PMID 24239329.
- Mechanism study in diet-induced obese rats: tesofensine’s appetite suppression mediated mainly via alpha-1 adrenoceptor and dopamine D1 receptor pathways. Axel, Mikkelsen, Hansen, Neuropsychopharmacology, 2010. PMID 20200509.
- Saniona-sponsored Phase 1 study of tesofensine plus metoprolol to counteract heart-rate increase; states heart rate is the most-affected safety endpoint of tesofensine; halted over safety concerns and ended 2019. NCT03488719.
- Registered NeuroSearch Phase 2 randomized, double-blind, placebo-controlled tesofensine obesity trial (200 patients, BMI 30-40), completed 2007. NCT00394667.
Regulatory status note: tesofensine is described here as investigational in the US with a favorable Mexican COFEPRIS technical-committee opinion in early 2023 and no approval in any country as of June 2026. Confirm current approval and filing status before publishing, as regulatory positions can change.



